27 January, 2026
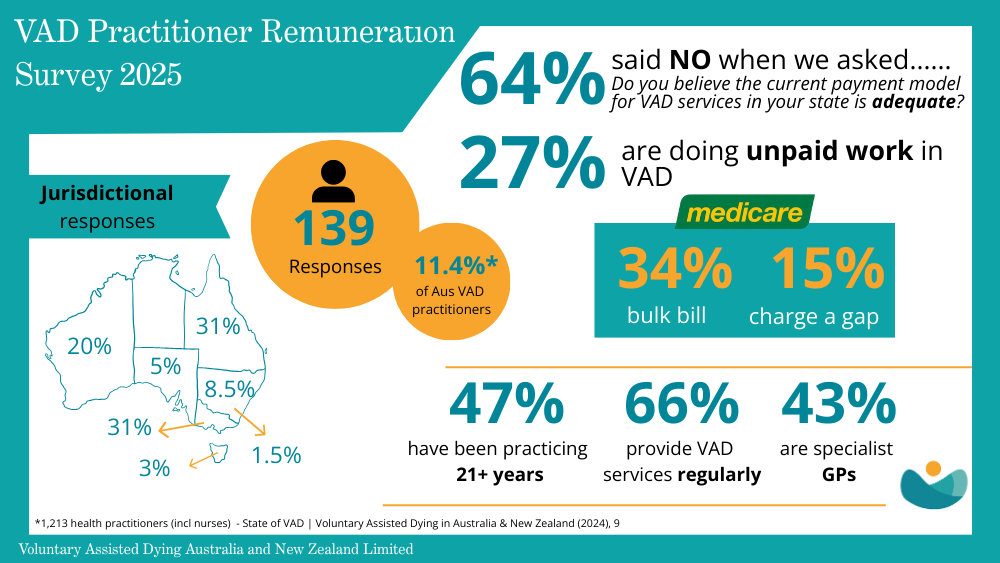
The 2025 VADANZ Remuneration Survey of VAD practitioners has revealed:
- Almost two‑thirds (63%) reported their state’s remuneration arrangements were inadequate.
- More than a quarter (27%) said they had provided unpaid VAD care.
- Only one‑third (32%) received any state government reimbursement.
- All respondents in South Australia and Tasmania reported dissatisfaction, as did 80% of Victorians.
- Queensland respondents were also largely dissatisfied (72%), particularly for rural and community-based doctors facing high travel burdens.
- New South Wales was the only jurisdiction where a slim majority (51%) felt remuneration was adequate.
 VADANZ President Dr Andrea Bendrups said VAD practitioners consistently report deep professional fulfilment in providing end-of-life care and remain strongly committed to supporting patients and their families. However Dr Bendrups noted that relying on goodwill made it difficult to maintain a stable and sustainable service over time.
VADANZ President Dr Andrea Bendrups said VAD practitioners consistently report deep professional fulfilment in providing end-of-life care and remain strongly committed to supporting patients and their families. However Dr Bendrups noted that relying on goodwill made it difficult to maintain a stable and sustainable service over time.
“All Australian jurisdictions, apart from the Northern Territory, have taken the courageous step of legalising VAD. Person-centered services have been established in all these jurisdictions which are delivering high quality end-of-life care, but relying on clinical altruism to do so. We urgently need to ensure those who provide this care have the support they need to continue doing so,” Dr Bendrups said.

At present, there are no dedicated Medicare items for VAD. The Medicare Benefits Schedule (MBS) excludes “euthanasia and any service directly connected to the procedure”, leaving practitioners uncompensated for extensive non‑clinical work such as administration, portal documentation, coordination, and travel.
Survey respondents told of the ethical discomfort they felt about charging privately for VAD services. However, without proper remuneration, many privately practising GPs and specialists face financial strain. Some practitioners are questioning whether they can continue providing VAD care long term.
“We are going to extraordinary lengths to shield patients from financial burden, but the system cannot rely indefinitely on the goodwill of practitioners,” Dr Bendrups said.
“This is not only a workforce issue, it ultimately affects patient access and continuity of care.”
Reduced practitioner participation risks limiting access to a compassionate end‑of‑life option, undermining continuity of care and compromising dignity and autonomy for patients.
VADANZ is calling for several reforms, including:
- Dedicated MBS items recognising the unique demands of VAD care.
- Comprehensive fee schedules covering all aspects of care, including travel.
- Increased numbers of funded hospital roles to provide stability for practitioners.
- Clear state guidance on billing options to reduce uncertainty.
- Federal updates to MBS Explanatory Notes to remove outdated restrictions on VAD items.
Dr Bendrups said the New Zealand model offers a proven template, with structured fee‑for‑service payments across five modules, additional remuneration for complex cases, and travel allowances. This system ensures transparency, fairness, and sustainability; principles that underpin a sustainable system.
“Without adequate remuneration, the system risks collapsing under the weight of unpaid labour and practitioner burnout,’’ Dr Bendrups said.
“We look forward to working constructively with policymakers to align funding structures with the realities of VAD practice.”